Emissions assessment across health care facilities in the Republic of Guinea
Categories: Net zero health systems, GHG emissions assessments, Country experience, Africa, Low carbon sustainable health systems
 Worshop for agents of health facilities in the Kankan Regional Health Inspection
Worshop for agents of health facilities in the Kankan Regional Health Inspection Country context
The Republic of Guinea is subdivided into four natural regions that are quite distinct from a geo-ecological point of view. These are: maritime Guinea (or Lower Guinea), Middle Guinea (or Fouta-Djalon), Upper Guinea and Forest Guinea. The differences between these regions are characterized by climatic contrasts, mountain barriers and the orientation of the reliefs. These differences combine to give each region particularities in terms of climate, soil, vegetation and lifestyle of the populations.
Guinea submitted, to the United Nations Framework Convention on Climate Change (UNFCCC), two national communications (2001 and 2018), its nationally determined contribution (NDC) in 2015, its National Strategy on Climate Change in 2019 and multiple other documents. However, no assessment of the climate footprint of the health sector had been carried out in Guinea before this project.
During the 26th Conference of the Parties (COP26) to the UNFCCC, Guinea, through the Ministry of Health and Public Hygiene (MSHP), took several commitments as part of the initiatives of the health program of said COP26 including, among others, the completion of the Baseline Assessment of the Greenhouse Gas missions of the health system, including supply chains.
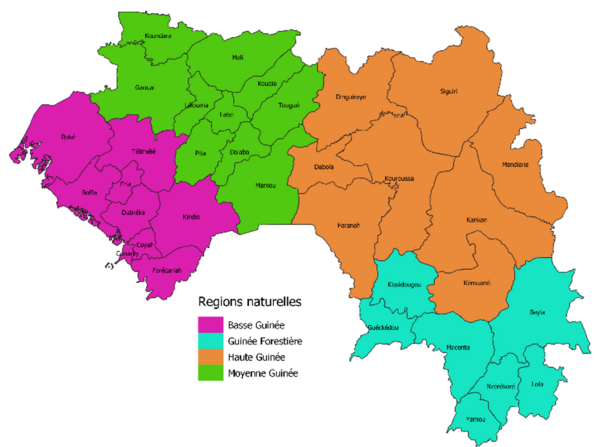
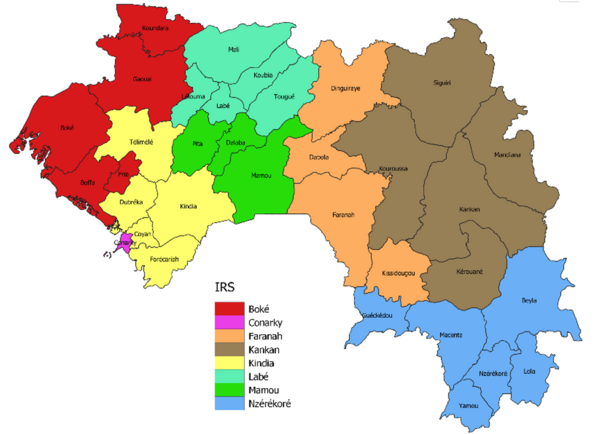
Maps of natural regions, Regional Health Inspections (IRS) and health districts of Guinea
Guinea carried out its last national inventory of greenhouse gas (GHG) emissions in 2020. On that date, Guinea's overall emissions were at 8699KtequCO2 including 4475 Kt CO2 for the energy sector, 357 Kt CO2 for the Electricity sector, 1441 Kt CO2 for the industrial sector in particular mining, 2421 Kt CO2 for the transport sector and 4 for the Household sector.
Internationally, it is known that the health sector generates a large number of GHGs which contribute to the climate crisis. However, no inventory or assessment of health sector emissions had been carried out in Guinea before this project.
Data on GHG emissions in the health sector is therefore of paramount importance for the government of Guinea in order to understand to what extent the health sector undermines or contributes to Guinea's capacity to meet its COP26 Commitments on climate change and health. These commitments are described as follows:
- Carry out a national vulnerability and adaptation (V&A) assessment of the effects of climate change on health;
- Continue to update the health component of the national adaptation plan (NAP) based on new evidence arising from assessments of vulnerability to the health effects of climate change;
- Conduct a baseline assessment of GHG emissions from the health system, including supply chains;
- Publish an action plan that sets out how we will develop a sustainable, low-carbon health system (including supply chains), taking into account the role that the health sector can play a key role, through its activities and actions, in reducing exposure to air pollution;
- Bring health sector emissions to zero;
- Use the V&A assessment, the HNAP and the action plan for a sustainable, low-carbon health system to facilitate access to funding intended to counter the effects of climate change on health.
Implementation process
Carrying out the baseline assessment of GHG emissions of the health system, including supply chains, is a key step in the implementation roadmap of COP26 commitments.
The general objective of the project undertaken in Guinea was to perform a baseline estimate of carbon emissions from Guinea's health system, including supply chains.
Specific objectives were to:
- Estimate carbon emissions from the health system by emission source;
- Estimate carbon emissions linked to supply chains;
- Determine the most polluting sources and health structures;
- Identify and/or propose possible measures to mitigate carbon emissions in the health sector.
To do this, a participatory approach with pedagogy was adopted, consisting of five steps or phases:




1. Definition of the scope of the evaluation: This phase consisted in defining the types and numbers of health facilities targeted for the evaluation, the objectives and strategic results of the evaluation, the stakeholders, the financial and human resources required to carry out the evaluation, the approach and the data collection and analysis tools. The year 2022 was chosen as the reference year and, after analyzes of data availability, it was agreed to use data from the period from 1is May to October 31, 2022.
2. Training on the Aga Khan Development Network tool: This phase led to the capacity building of two experts from the Country Office of l’WHO-Guinea, four national experts (2 from the MSHP and 2 Ministry of Environment and Sustainable Development (MEDD)) and 60 agents from 60 health facilities on the use and exploitation of the tool carbon assessment and management in the health sector (AKDN), a total of 66 people through the organization of 5 training workshops in regional health inspections: Conakry, Kindia, Labé, Kankan and N'Zérékoré. Targeting health workers from health facilities to carry out data collection, with the involvement of those responsible for said health facilities, promotes the sustainability of the process with the prospect of strengthening self-assessment capacities.
3. Data collection: The data used to estimate GHG emissions from Guinea's health system were collected in 51 health facilities (2 university hospital centers (CHU), 7 regional hospitals, 26 prefectural hospitals, 7 Communal Medical Centers, 7 private clinics and 2 company hospitals). This collection was made using the health carbon assessment and management tool AKDN/WHO.v1.6.2. At the beginning, it was planned that the data would be collected in the 60 large health structures in the country, but during the data collection, it was noted in the field that out of these 60 target health structures, 9 did not have data. reliable over the reference year.
4. Validation, processing and analysis of data: The data collected in the health facilities were validated by the restricted group of experts and representatives of the target health facilities. After this validation, taking into account the limited capacity of the AKDN tool (30 health facilities or buildings maximum) the data from the health facilities (buildings) were compiled in the sub-files of the AKDN tool according to the categories of health structures. : University Hospitals, Regional Hospitals (HR), Prefectural Hospitals (HP), Communal Medical Centers (CMC) and Private Clinics (CP).
5. Development and validation of the report on carbon emissions in the health sector: After analyzing the data, we proceeded to interpret the graphs and data, propose GHG mitigation options as well as 'to the writing of the study report. After its validation, the report was edited and shared with the MSHP authorities and with the 51 health facilities. The next steps are: (i) development of the national carbon footprint mitigation plan for the health sector (PNACS); (ii) mobilization of resources for the implementation of the PNACS; updates of the assessment of GHG emissions.
Results

The assessment of GHG emissions in Guinea's health system made it possible to obtain the following results:
- Annual greenhouse gas emissions from the health sector of the Republic of Guinea, including supply chains, were estimated at approximately 14,337.8 tonnes of carbon equivalent (CO2eq) i.e. an average footprint of 39.8 tonnes CO2eq per day. These emissions are unevenly distributed between the three fields of application (“scopes”), as presented in Figure 3.
- Scope 1 emissions, i.e. annnual emissions resulting directly from the activities of health facilities of Guinea's health sector amount to approximately 5002.2 tonnes CO2eq. The main sources of direct emissions identified are: refrigerant gases, generators, service vehicles (transport of staff and patients), healthcare waste and anesthetic gases.
- Scope 2 emissions, i.e. indirect emissions resulting from the services provided to health facilities by local private or local public companies, were estimated at approximately 917.1 tonnes CO2eq. The main source identified is energy obtained from the Electricité De Guinée (EDG) company.
- Scope 3 emissions, i.e. those coming from other entities that provide products or services contributing to the performance of health facility operations, were estimated at approximately 8418.4 tonnes CO2eq per year. The main sources of emissions identified in this scope are: professional travel and public transport missions (Taxi, plane), Inhalers, healthcare waste transfers to SMEs and the supply chain. Emissions linked to the supply chain are estimated at approximately 7996.0 tonnes CO2 eq per year. The main data or information used to estimate supply chain emissions relate to costs linked to: purchases of anesthetic gases, purchases of certain pharmaceutical products from certain private suppliers, purchases of consumables and laboratory equipment as well as the cost of maintaining the installations.
- 46 action areas to mitigate or reduce GHGs were proposed, based on the information drawn from the analysis of data and the main sources of emissions identified in the health system. These include: seven actions in the area of refrigerants, nine in the area of energy, eight for transport, three in the area of supply chains, five in the area of research and nine to promote the integration of the dimension of climate change into policies and public health programs. These courses of action will serve as a basis in the development of the national plan to mitigate carbon emissions in the health system, including local and specific measures to be taken by health facilities.
Lessons learned
During the assessment, several success factors and challenges were identified as lessons learned.
Success factors
The following elements were most effective in advancing the GHG baseline assessment in the Republic of Guinea:
- Adoption of a participatory approach with pedagogy: the involvement of the main stakeholders in the health sector, strengthening their capacities and raising their awareness of the importance of each in the process of implementing COP26 commitments ;
- Organization of a stakeholder consultation workshop by the Ministry of Health and Public Hygiene (MHSP), with the support of the WHO, on the issues of climate change and health, which led to the identification of technical services and the official designations of respondents of these structures for the implementation of COP26 commitments;
- Formal designation of a focal point on climate change and health within the MSHP;
- Empowerment of the National Directorate of Public Hygiene (DNHP) as the technical service of the MSHP responsible for implementing the COP26 commitments of adaptation and mitigation in the health sector in the face of climate change. For example, in the decree relating to the attribution and organization of the DNHP, it is mentioned that the DNHP is the structure responsible for implementing the commitments made by Guinea on health and climate change but also for the integration of climate change in Guinea's health policies;
- Carrying out a stakeholder analysis and developing the roadmap for the implementation of COP26 commitments;
- Involvement of managers of health facilities and health authorities at all levels, particularly during data collection and validation of data, the proposal of possible solutions and validation of the report.
Challenges
The following challenges and areas of improvement were identified:
- Operationalization of National Working Group: During the analysis of stakeholders for the implementation of COP26 commitments, a National Working Group on Climate Change and Health was set up for the occasion. It had been requested that the Ministers in charge of health and the environment issue a joint decree to formalize and make this group operational, but this decree has not been signed until now, which has impacted the mobilization of certain services.
- Increased mobilization of funds: The funds that were mobilized to carry out this evaluation were insufficient, which led to very prolonged interruptions of consultation contracts, the failure to take into account health centers and certain aspects in the evaluation, but also delays in the implementation of activities. To avoid this type of situation, a substantial and sufficient mobilization of funds would be needed from the start, to take these aspects into account.
- Health facilities involvement: In this evaluation, the health facilities that were evaluated were not involved in the definition/proposal of GHG mitigation action options due to limited resources. This is why, in view of the role that health facilities must play in the implementation of GHG mitigation actions, it would be even better if the staff of these health facilities were more involved in defining and prioritizing GHG mitigation action options.
- Scope of the assessment: One of the limitations of this evaluation is that it does not take into account emissions from health centers, technical services, or the MSHP office. It would have been better if the assessments of GHG emissions were extended beyond health centers to technical services and the MSHP office.